
The distribution of drug from plasma to target tissues can be effected by a number of factors but perhaps the most important is Plasma Protein Binding (PPP). Compounds that are extensively bound to plasma proteins will have a low Volume of distribution (Vdss), can have long plasma half-lives (T1/2), and have low clearance (Cl) by both liver (hepatic) and kidney (Renal) routes.
Assay
Compounds are incubated in plasma for 1 hour, then centrifuged at 2700 rpm 10 mins. The supernatant is then analyzed for drug concentration, results are usually expressed as percent bound. The experiment can easily be carried out with plasma from different species.
Until the drug is greater than 90% bound there is not usually any issues, once you get to >99% bound then plasma protein binding is likely to have a significant impact.
Strategies
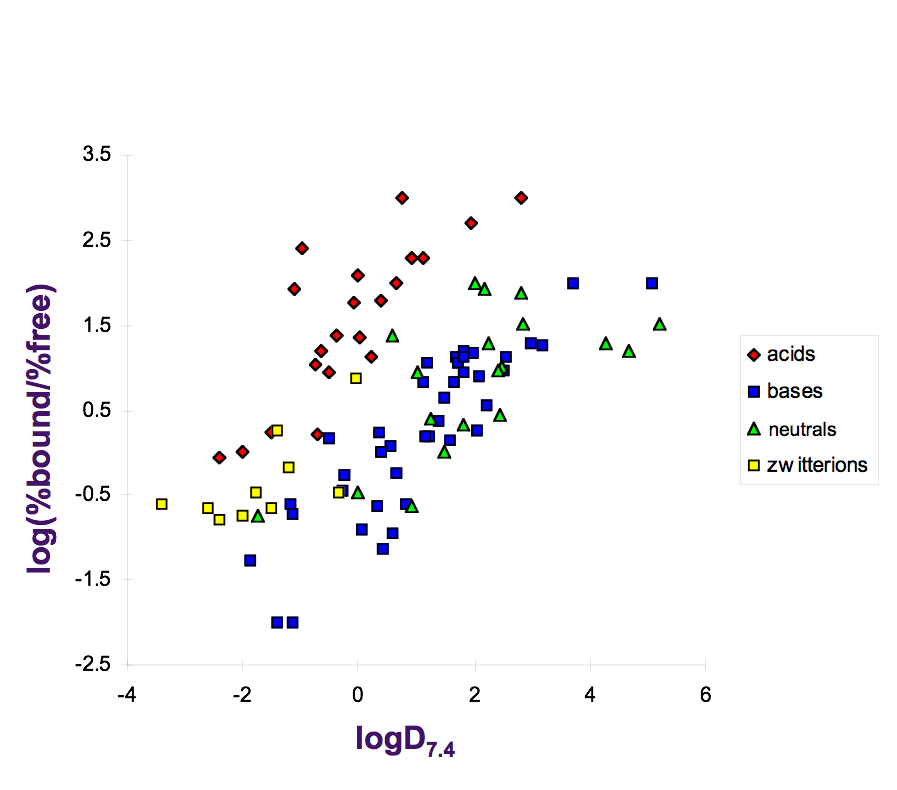
Different classes of compounds are more likely to have problems with PPP, acids tend to display the highest affinity for plasma proteins as shown in the graph below (taken from the talk by Rupert Austin at the RSC MedChem School). The graph shows a plot of log(%bound/%free) versus LogD. In general the more lipophilic compounds display greater plasma protein binding, in the case of acids compounds with LogD > 0 are almost all >99% bound. Neutral and basic molecules usually require LogD greater than > 4 before plasma protein binding becomes an issue.
The major plasma proteins that can interact with drugs are:
- Albumin
• Alpha-1-acid glycoprotein
• Lipoproteins
In general, acidic and neutral drugs primarily bind to albumin, and basic drugs bind to the acidic alpha-1 acid glycoprotein.
Albumin, (HSA) is the most abundant protein in human blood plasma. It is produced in the liver. Albumin comprises about half of the blood serum protein, (30 to 50 g/L). There are almost 100 crystal structures of albumin, 58 with ligands bound, in the Protein Database PDB. An example is 2vdb in which S-Naproxen is bound.
Alpha-1-acid glycoprotein, (AAG, AGP, Orosomucoid, ORM ) has a normal plasma concentration between 0.6-1.2 mg/mL (1-3% plasma protein). It is negatively charged at physiological pH and interacts mainly with acidic drugs, including beta-adrenergic-receptor blockers, antidepressants, neuroleptics and local anaesthetics. There is a single crystal structure in the PDB 3bx6, the branched, partly hydrophobic, and partly acidic cavity, together with the presumably flexible loop 1 and the two sugar side chains at its entrance, explains the diverse ligand spectrum of AGP, which is known to vary with changes in glycosylation pattern.
Binding of some drugs to plasma proteins
Albumin
Ceftriaxone (A)
Clindamycin (A)
Clofibrate (A)
Dexamethasone (N)
Diazepam (N)
Diazoxide (A)
Dicloxacillin (N)
Digitoxin (N)
Etoposide (N)
Ibuprofen (A)
Indomethacin (A)
Nafcillin (A)
Naproxen (A)
Oxacillin (A)
Phenylbutazone (A)
Phenytoin (A)
Probenecid (A)
Salicylic add (A)
Sulphisoxaole (A)
Teniposide (N)
Thiopental (A)
Tolbutamide (A)
Valproic acid (A)
Warfarin (A)
Albumin and AAG
Alprenolol (B)
Carbamazepine (N)
Disopyramide (B)
Erythromycin (B)
Lidocaine (B)
Meperidine (B)
Methadone (B)
Verapamil (B)
Albumin and Lipoproteins
Cyclosporine (N)
Probucol (N)
All
Amitriptylline (B)
Bupivacaine (B)
Chlorpromazine (B)
Diltiazem (B)
lmipramine (B)
Nortriptyline (B)
Perazine (B)
Propanolol (B)
Quinidine (B)
A=Acid; B=Base ; N=Neutral.
Note that only unbound fraction of the drug undergoes metabolism in the liver and other tissues.
Last Updated 21 Sept 2009
See also Transporters
Back to ADME Properties
Back to Drug Discovery Resources